Wines get better with time-they say-but the same can’t be said with old hypotheses unsupported by good evidence. Hypothesis in question is that of dietary protein restriction in management of CKD. With the expanding armamentarium of CKD, when nephrologists were almost saying goodbye, the protein restriction debate was sparked by the latest KDOQI (2020) guidelines, by recommending Very Low Protein Diet (VLPD) (0.3-0.5gm/kg/day) with ketoanalogues in patients with pre dialysis CKD (1A recommendation). Debate was colored further by the NEJM review article as many doctors believe that the letters printed on those glossy color pages of the journal are as sacrosanct as religious texts of Bhagavad Gita or New Testament. For academic atheists like me, however, it’s a difficult pill to digest.
Absence of enough evidence, possibility of harm, old, non contemporary nature of the evidence and better things that one can try in patients with CKD are the principal reasons why the idea of protein restriction is useless in current practice. We recently reflected upon this issue in a review which just underlines the famous quote by F Parsons-all a low protein diet does is to shrink the patient down to the size of his kidneys. VLPD may postpone the decision to start dialysis for a few months while increasing the risk of malnutrition and death in the bargain.
Obesity and metabolic syndrome are precursors of the two most important CKD risk factors-diabetes and hypertension. They elevate CV risk manifolds and mitigation of this risk doesn’t need complex dietary plans but simply the restriction of salt, sugar and fat. This trio arguably underlies the major death toll, far greater than that of all the wars and natural calamities put together. Most of our patients don’t want to be bothered much about these: we know that, just talk about a diet for creatinine! Why we prefer to remain blind to the obvious and keep searching for illusory solutions in the diet is beyond comprehension. Probably, we feel so badly about salt, sugar and fat, that we simply love them!
CKD Diet: with a pinch of humor
Visit to the nephrologist is incomplete without the discussion of diet-that’s what most patients in India believe. Many patient families hold a strong opinion (opinions are not the monopoly of guideline experts) that diet is far more important than medications, optimum blood pressure control, physical activity and moderation of caloric intake. As the menu of questions concerning CKD diet is far more diverse than that of an average Gujarati Thali, these diet talks exceed the typical time needed for the actual consultation.
These sessions are greatly enjoyed by patients and families alike but are often irritating to the doctors and for the next patient waiting outside the chamber. As if this was not enough, even other specialist colleagues tell patients to ‘get the diet clarified by the kidney doctor’ as if the food eaten is metabolized by the kidney and nephrologists are in possession of additional qualification in nutrition science! I usually teach such colleagues a lesson by making sure that patient doesn’t see them back ever again(just kidding!).
So let’s see what CKD diet is. Only thing that is clearly known about this diet is that it’s never the same for 2 different patients. Take for instance, the happy couple of Hansaben and Mukeshbbai, whom I saw in OPD at the beginning of my practice. Mukeshbbai, a gentleman in his 80s, with well controlled diabetes and hypertension, was rushed to my office after discovering that his eGFR has dropped to 60. Hansaben was a lady of discipline, and had taken over management of the kitchen after Mukeshbbai got to know about his kidney problem. After assessing his case, I assured the couple that the kidney problem isn’t that serious and you can be less restrictive about his diet.
This information came as a disappointment and relief for Hansaben and Mukeshbbai respectively. Mukeshbbai was specifically fond of the ‘tomato-uttapam’ which (in addition to other tomato containing foods) was banned completely in his diet for over a year. When I said that tomatoes won’t harm the kidney, Mukeshbbai was in tears, reflecting how deeply he loved that tomato uttapam. I was very happy to have helped him but this joy was short-lived as Mukeshbbai stopped seeing me thereafter. Surely Hansaben wasn’t happy with my ignorance about the intricacies of the CKD diet. However, Mukeshbbai, although now under the care of a different nephrologist, sees me once in a while (of course secretly) just to say thank you, while returning back from that famous South Indian food joint!
Mukeshbbai got his tomato uttapam back, but I lost a patient. What is the use of the knowledge or the facts about the diet if that is going to take away your patients? Instances like these were so annoying in my initial practice that I was on the verge of being burnt out. But a senior nephrology colleague saved my life. I happened to attend his interesting lecture which literally enlightened me about CKD diet.
First of all, he said, you have to actually come to share the belief that the “CKD diet” is the most important aspect of clinical practice although all of us are well aware that it’s sham. This is in the interest of maintaining your sanity in the practice and keeping your clientele. Second, it is best to remain passive and patient in these discussions, saying less and listening more. This, however, doesn’t mean that you appear unsure/uncertain. A rule of thumb in practice is that the certainty of your advice should generally be inversely proportional to the strength of evidence on which it is based. Whether bajra roti is better than jowar roti or if seeds should be taken out of the capsicum or boiling dal at 100 degree centigrade for 20 min would be better than 80 degrees for 40 min, baby brinjal versus giant brinjal,-whatever the question may be, it’s far more important to be sure than correct. Don’t ever say that ‘either of these is ok’; as this will leave the patients restless and invite 10 more questions that were previously not on his/her question list (yes, like home BP chart, patients carry this always). Careful listening to each case will eventually help you understand the “CKD diet” of your patient-each one may have a little similarities-but is always unique, thanks to the rich vegetation and flora of our country.
He emphasized the need to understand this area of our practice as a blessing in disguise. For example, a patient with diabetic nephropathy, experiencing steady decline in kidney function in spite of the best of your efforts. This is not a very comfortable scenario, when a patient, with his anxious daughter and son in law, are staring at you (when you are cluelessly going through all his previous records) with expressions showing variable proportions of hope, fear and anger. A nephrologist often feels cornered in this situation, with no clue as to how to break the ice, when daughter offers a respite by recalling that father ate 3 samosas at an anniversary party last week. You are relieved (that’s why I love this snack!), for at least another month until the next follow up.
Finally, he narrated a story of a very senior physician who held very rigid and peculiar views about food and health, which in nutshell, summarized the CKD diet. The man in question had a roaring practice and saw hundreds of patients in a day. One of his recommendations was complete avoidance of bottle gourds/Dudhi. Being a very authoritarian figure, no one dared to question his peculiar dietary recommendations, and patients and doctors remained clueless about the rationale, which was to be inadvertently revealed by alcohol. In a party where he was celebrating his 80th birthday, after a couple of drinks, one of his students dared to ask him this question,”What is wrong with Dudhi in diet?”
“Nothing, I just hate Dudhi!”
Now, you can replace Dudhi with Chicken, Capsicum, Tomato or any damn thing and come with a customized CKD diet of your own. Moral of the story is that dietary recommendations are driven more by such personal biases than credible scientific evidence.
May you be in private or academic practice, there is no getting away from the devil-CKD diet. So as don Carlene has famously said,”Keep your friends close, but enemies closer”.
It is believed that conventional diffusion-based dialysis is not effective to remove larger-molecular-weight toxins. In contrast, hemodiafiltration (HDF) uses convection to remove broad range of uremic toxins and may improve patient outcomes. CONVINCE trial was a multinational, randomized, controlled trial that compared the benefits of high-dose hemodiafiltration (HDF) with standard hemodialysis (HD) in adult patients with end-stage renal disease (ESRD). A total of 1360 patients were randomized to receive either high-dose HDF or high-flux HD.
The intervention group received high-dose HDF with on-line production of substitution fluid and bicarbonate-based dialysis fluid at a convection volume of at least 23 liters per session in the postdilution mode. The control group received conventional dialysis with a high-flux dialyzer. Median dialysis vintage of enrolled patient was around 3 years.
The primary outcome was death due to any cause. After a median follow-up of 30 months, high-dose HDF resulted in a lower risk of death (17.3%) than conventional high-flux HD (21.9%) (hazard ratio [HR], 0.77; 95% CI, 0.65-0.93).
At first glance, the trial appears to provide unequivocal evidence of the benefit of HDF over HD. However, there is a caveat. The treating physicians may have enrolled patients who were likely to have reached a convection volume of 23 liters. These patients were likely to be healthier than the average patient with ESRD. It can be recalled that median dialysis vintage was 3 years. The mortality rate was lower than expected in both groups.
Overall, the CONVINCE trial provides evidence that high-dose HDF may be associated with a lower risk of death than conventional HD in patients with ESRD. However, the results of the trial should be interpreted with caution, as the study population may have been healthier than the average patient with ESRD. It remains to be seen what would happen if incident dialysis patients were enrolled. The magnitude of benefit may not replicate in all patients. Also, widespread application of HDF demands additional resources in terms of ultrapure water, HDF machines and technical expertise.
Short-Course Antibiotic Therapy for Uncomplicated UTI in Children(SCOUT TRIAL)
SCOUT was a randomized, controlled, non-inferiority trial that evaluated the efficacy of short-course antibiotic therapy (5 days) versus standard-course antibiotic therapy (10 days) for uncomplicated urinary tract infection (UTI) in children aged 2 months to 10 years.
Children who showed clinical improvement after 5 days of therapy were randomized to receive either another 5 days of antibiotics (standard course) or 5 days of placebo (short course). The primary outcome was treatment failure, which was defined as symptomatic UTI at or before the first follow-up visit at 11 to 14 days.
Of 664 randomized children, primary outcome occurred in 0.6% (2) children assigned to standard course and 4.2% (14) children assigned to short course. This means that treatment failure was 7 times more common in the short-course arm. The absolute difference was 3.6%.
The non-inferiority margin specified was a difference in absolute rate of treatment failure of more than 5%. In other words, the primary non-inferiority analysis evaluated whether there was a greater than 5% increase in the absolute risk of treatment failure in children assigned to short-course therapy compared with children assigned to standard-course therapy. The upper bound of the 95% confidence interval (CI) was 5.5%, which was below the non-inferiority margin. Therefore, the study did not prove non-inferiority of short-course therapy compared to standard-course therapy.
Some aspects of the trial are to be highlighted. One, though the distinction between cystitis and pyelonephritis is difficult in children, short course might be sufficient for cystitis. Two, there is differing follow up times to assess treatment failures for two arms. Both the arms were followed up for primary outcome at same time while the antibiotic would have been stopped earlier for the short course group.
SCOUT was a well conducted trial, but the evidence generated does not convince us that a short course is sufficient to eradicate infection. Though the authors conclude “short course is a reasonable option”. We are skeptical about this option. Duration of antibiotics must be decided on case-to-case basis and after discussing with care givers regarding risks and benefits of short course antibiotics.
Management of hypertension is one of the most important tasks of nephrologists, which if done well can be highly rewarding. More often than not, blood pressure is either left uncontrolled or is lowered too much, putting patients at risk of the attendant complications. Realising the fallacy and dangers of ‘one size fits all’ approach which has been the part of preexisting guidelines, ACC/AHA 2019 guidelines, were a much needed departure from the ‘target based’ to the ‘risk based’ approach of BP treatment. This is a sensible approach, when one views BP elevation as a risk factor for organ damage/dysfunction and not a disease in itself, with lesser emphasis on moving a BP number from a higher to lower value and greater emphasis on reducing the risk posed by elevated BP to the health.
However, KDIGO 2021 HTN guidelines seem to be traveling back in time to embrace the target blood pressure, the magical number <120 systolic for the entire CKD population (except those on dialysis).
This recommendation not only lacks sufficient evidence, but if implemented strictly by treating doctors, can be potentially disastrous. A recent review has summarised the serious limitations of the evidence on which KDIGO 2021 BP target is based, and we will discuss here the basis for more conservative BP targets for most patients with CKD.
Why is BP elevated in patients with CKD?
Blood Pressure=Cardiac Output x Systemic Vascular Resistance
Given the fact that most patients with CKD will have high BP, what factors elevate CO or SVR in these patients?
Disturbance of sodium and volume regulation (not appreciable as edema in early CKD), activation of RAS and sympathetic nervous system, anemia and multiple other factors determine BP by affecting CO or SVR. This makes hypertension in CKD pathophysiologically complex and different from primary hypertension(figure 1). Therefore, the data guiding treatment of primary hypertension can’t be directly extrapolated to HTN in CKD. Hypertension is not a disease in itself but a risk factor for organ damage/dysfunction and consequent morbidity and mortality. Risk with hypertension in CKD is two folds: cardiac plus renal. One also needs to acknowledge the nature of CV disease in CKD which isn’t all the same as the general population without kidney disease. Uncontrolled BP is one of the most important determinants of CKD progression along with proteinuria, and multiple pivotal trials in diabetic CKD –Captopril trial, RENAAL, IDNT-(although they were not BP target trials) have shown the efficacy of antihypertensive therapy in renoprotection.
Figure 1. Pathogenesis of hypertension in chronic kidney disease
Limited generalisability of SPRINT CKD to the real world CKD
Data supporting BP target of <120 systolic comes from SPRINT trial.
First of all, one needs to understand that SPRINT-CKD, unlike EMPA-KIDNEY or DAPA CKD, isn’t an independent randomised controlled trial, and is a pre-specified subgroup analysis of SPRINT trial.
If you wish to prepare a checklist of ‘refer to nephrology’ for a primary care doctors clinic, you may rather copy paste SPRINT trial exclusion criteria which go like this: diabetes, proteinuria >1gm/day, ADPKD, glomerulonephritis, eGFR <20 (in addition to age <50). Mean serum creatinine in this elderly population (age 67 yrs), was 1.56mg/dl, and urinary albumin excretion was ~40 mg/gm. This clearly is not a ‘nephrologist’s patient population’, unless the physician is a very good friend of yours or is too scared by serum creatinine of 1.56mg/dl in an elderly non diabetic. Indeed, the rate of eGFR decline in SPRINT trial is similar to the age associated decline in kidney function. Extrapolating findings from SPRINT CKD cohort to CKD clinics is going to be a mistake that can cost (mostly borne by kidney).
The conclusion of the SPRINT CKD goes like this:
“among patients with CKD and hypertension without diabetes, targeting an SBP<120 mm Hg compared with <140 mm Hg reduced rates of major cardiovascular events and all-cause death without evidence of effect modifications by CKD or deleterious effect on the main kidney outcome” . Even authors themselves (and rightly so) don’t claim to have established a new BP target for CKD. These findings only mean that main SPRINT results are also applicable to the ‘accidental CKD’ like the rest of the population.
Accidental CKD is detected when an elderly patient with comorbidities gets to know that he has CKD after reading the eGFR value in the bold type which at the bottom of the paper also gives the latest KDIGO CKD classification. Telling them “nothing to worry about” and seeing the wrinkles disappear from their faces is one of the happy moments in our practice. This age associated decrease in GFR without significant albuminuria is of questionable significance and is arguably the medicalisation of aging.
Limited generalisability of the SPRINT CKD was highlighted by a study performed across 40 Italian nephrology clinics, involving 2847 patients. This population differed significantly from the SPRINT CKD, specifically, they have higher risk of ESRD, CV deaths and all cause mortality.
Intensive BP lowering may be harmful
An important concern for the broader application of <120 is the harm, and this is particularly relevant to the CKD. Two trials that dealt with a very similar BP target in diabetics and non diabetics (ACCORD BP and SPRINT) reached discordant primary outcomes, however, they concur upon the harm of intensive BP lowering.
In the ACCORD BP trial, serious adverse events attributed to BP lowering were more likely in the intensive lowering arm: hypotension, syncope, bradycardia/arrhythmias. Importantly, in a population at very low risk of progressive CKD (mean creat 0.9mg, median UACR 14mg/gm), risk of of eGFR <30ml (as an adverse lab measure) was doubled with intensive BP lowering [99 (4.2%) vs 52 (2.2%) <0.001]. Alarmingly, renal failure occurred in 5 patients in the intensive control arm versus 1 patient in the less intensive arm.
In SPRINT trial as well, in addition to increased risk of hypotension, syncope and electrolyte abnormalities, intensive lowering led to higher incidence of AKI [204 (4.4%) vs 120 (2.65) HR 1.71 P<0.001], ≥30% reduction in estimated GFR to <60 ml [ 127 (3.85) vs 37 (1.1%) HR 3.49 P<0.001].
A post hoc analysis of SPRINT showed a higher risk of AKI and eGFR based renal outcomes (≥30% decrease in eGFR to a value of <60 mL for participants without CKD; and a composite of ≥50% decrease in eGFR the development of ESRD with CKD) in the intensive control group. This analysis also showed that the CV protective effect of intensive BP lowering is significantly blunted at reduced GFR and was no longer significant at eGFR<45 ml per min(figure 2,3,4).
Figure 2. Risk of AKI is higher in patients with eGFR <45 ml/min( J Intern Med 2018 Mar 283(3):314-327)
Figure 3. eGFR based renal outcomes (≥30% decrease in eGFR to a value of <60 mL for participants without CKD; and a composite of ≥50% decrease in eGFR the development of ESRD with CKD) is higher in intensive BP control group (J Intern Med 2018 Mar 283(3):314-327)
Figure 4. CV protective effect of intensive BP lowering is blunted at reduced GFR and was no longer significant at eGFR<45 ml per min (J Intern Med 2018 Mar 283(3):314-327)
Many patients in nephrology clinics have severe hypertension, often symptomatic with headache, visual disturbances (This is another dark room in nephrology awaiting to be lit). These patients are younger and don’t have other traditional CV risk factors like dyslipidemia or atherosclerotic CVD. How will this group fare with intensive BP lowering? An interesting analysis using patient-level data from 9361 randomised participants of SPRINT trial evaluated a similar issue. They studied the impact of baseline BP and Framingham risk score on outcomes, and showed that in participants with a baseline SBP of at least 160 mmHg and a lower Framingham risk score, targeting an SBP of less than 120mmHg compared with less than 140 mmHg resulted in a significantly higher rate of all-cause death [hazard ratio (95% CI) for intensive group: 3.12 (1.00-9.69); P = 0.049].
SPRINT trial was terminated early after 3.5 years, and therefore the long term impact of these renal events on CKD outcomes remains a question and there is no reason to believe in long term safety of intensive BP control. Premature termination of RCTs carries the risk of overestimating the benefits and underestimating the harm of the intervention. What will happen to this renal function decline over years of follow up? The correct answer to this question is “we don’t know”. However, KDIGO prefers to dismiss it as a hemodynamic and transient phenomenon. Although ‘nephrotoxicity’ of intensive BP lowering hasn’t bothered trialists and KDIGO guideline makers, the risk benefit of intensive BP lowering needs to be carefully discussed with our patients before implementation.
Why was there a dissociation between CV and renal benefits in SPRINT?
Figure 5. Spectrum of risk factors for CV events changes with progression of CKD
Is ‘some renal compromise’ an inevitable consequence if you wish to gain CV benefits? We believe that this apparent ‘cardiorenal paradox’ has to do with the different nature of CV risk profile in CKD. With worsening kidney function, the nature of CV risk changes, with greater contribution from non-traditional CKD specific risk factors (in addition to traditional atherosclerotic CV risk factors)(fig 5). CKD in a nephrologist’s clinic resembles more to the participants in the landmark CKD-BP trials: Captopril study, REIN , RENAAL and IDNT, MDRD and AASK. Unlike SPRINT or SPRINT-CKD, most of these trials dealt with participants having high risk of CKD progression. In such patients, renoprotection is likely to go hand in hand with cardioprotection, and intervention in addition to kidney disease is likely to offer cardioprotection as well (considering the fact that CV disease in this population is often non-coronary i.e. left ventricular hypertrophy, systolic and diastolic dysfunction, and cerebrovascular disease).
Is KDIGO recommendation valid if standardised BP measurement is universally adopted?
One argument put forth in support of intensive BP lowering is that if we measure BP properly (standardised office BP or AOBP) and minimize white coat effect, a target of <120mmHg will make sense.
We argue that even if one imagines a theoretical scenario where AOBP will be used universally for monitoring BP, intensive BP lowering will still have all the attendant risks that we discussed. In a systematic review and meta analysis, involving 9279 participants, AOBP readings were 7-14 mmHg lower (the difference in the routine office BP and “research settings” was ~7 mmHg and that between routine office and AOBP was 14 mmHg). Even if we adjust for the way BP is recorded, none of the pivotal CKD trials (even post SPRINT) had reached target SBP <120 mmHg(table 1).
Clinical trial
Blood pressure achieved (intervention vs control)
Captopril
128-134 vs 129-136
IDNT
141/77 vs 144/80
RENAAL
140/74 vs 142/74
CLICK
130/70 vs 140/75
DAPA CKD
??? vs 137/78
EMPA KIDNEY
control arm BP 137/78 (Reduction in SBP was−2.6 mm Hg in intervention)
Table 1. List of randomised control trials on CKD patients. with serum creatinine values at the enrolment and target BP achieved in the trial. As can be seen, even in the research settings the target BP of 120 mmHg was not achieved in landmark trials involving patients with CKD
What do we already know about BP targets in CKD?
Before SPRINT-CKD, what did we know about intensive BP lowering in non diabetic CKD? Two trials that evaluated the effect of intensive versus less intensive BP targets in real world non-diabetic CKD are MDRD (serum creatinine 2-3 mg/dl) and AASK (serum creatinine 2-2.2mg/dl, >30% participants had UACR >0.22). Both assessed impact of this intervention primarily on kidney function, as decline in eGFR, and concluded that lower target (<125 in MDRD, <129 in AASK) doesn’t offer additional renoprotection than usual targets. Subgroup analysis of patients with proteinuria suggested the benefit of lower target on kidney outcomes. Post trial follow up of AASK and MDRD (for 14-15 years) claimed reduced overall mortality (HR 0.87, 95% CI 0.76-0.90), and also reduced the progression to ESRD (HR 0.88, 95% CI 0.78-1.00), but the benefit was confined to those with proteinuric CKD. These findings from post trial follow up should be interpreted with caution: they are discordant with primary outcome of the original trials, observed differences in outcomes are marginal, and importantly, there was no difference in the blood pressure between the groups in the follow up period. Several meta-analyses combining these trials of various designs, interventions, different BP targets, not surprisingly, have reached different conclusions claiming (here and here) and refuting (here and here) the benefit of intensive BP lowering.
Nephrology dark room
Figure 6. There is a lack of data about BP targets in advanced CKD, X axis depicting serum creatinine concentration of the trial population
Even the landmark BP-CKD trials have involved the patients with mild to moderate decrease in kidney function and evidence guiding BP treatment in more severe CKD (and not on dialysis) is virtually nonexistent (figure 6). Unfortunately, KDIGO doesn’t make any distinction about the advanced CKD (which may be one of the most prevalent patient populations in nephrology OPDs), implying that target <120 is valid across the spectrum of CKD.
What should clinicians do in the absence of convincing evidence for BP goals in their patients? Patient’s values and preferences should be considered while developing guidelines, KDIGO committee didn’t have patient representation. What would patients with CKD value? Patients and clinicians may believe that intensive BP lowering reduces all cause mortality significantly (relative risk reduction of 28%), however they need to be informed about a much smaller absolute risk reduction of 1.9%. On the basis of SPRINT results, for every 1000 patients treated for 3.2 years with intensive BP lowering compared to the less than 140 systolic, on average, 19 persons will benefit, 26 will experience acute renal failure (ARF),*955 will not experience benefit or harm. Such clear discussion of the risk-benefit should be done with all those patients in whom intensive BP lowering is considered. In our CKD clinic, after screening 119 patients, 12 met inclusion criteria, of which only 2 agreed to go for the intervention of intensive BP lowering (unpublished data, Tukaram Jamale).
*ARF was the terminology by SPRINT trial in adverse event reporting. It’s interesting to know how this trial defined acute kidney injury. ARF was included as an event if the diagnosis was listed in the hospital discharge summary, and considered by the SPRINT Safety Officer, after reviewing medical records to be one of the top three causes of the admission or continued hospitalization. A few patients with ARF were noted in the emergency department records instead of hospitalization records.
In the opinion of the KDIGO committee, if there is uncertainty about the risk/benefit, it seems ok to consider the benefit and ignore risk. See a paragraph from the guideline document below:
Is there a plausible mechanism of harm?
In patients with long standing hypertension and especially those with comorbidities like CKD, the pressure-flow curve of the blood flow in various organs (e.g. brain) is shifted to the right(figure 7).
Figure 7. In hypertensive patients, the autoregulation curve is shifted to the right.
In other words, the blood pressure threshold that leads to compromised tissue perfusion in hypertensive patients is different (higher) than the general population. Importance of this phenomenon was highlighted in several studies involving patients with chronic hypertension seen in acute care settings. For example, SEPSISPAM trial, that evaluated two different MAP targets in patients with sepsis (80-85 vs 65-70 mmHg), primary outcome of 28 day mortality didn’t differ in the two groups, however, among patients with chronic hypertension, those in the high-target group were less likely to experience the doubling of serum creatinine [90/173 (52.0%) vs 65/167 (38.9%) p=0.02] and required less renal-replacement therapy [73/173 (42.2%) 53/167 (31.7%) p=0.046] than those in the low-target group. Another trial involving peri operative patients evaluated individualized versus standard BP management strategy (aimed at achieving a SBP within 10% of the patient’s resting SBP vs treating when it falls below 80 systolic), individualized management was associated with a non significantly reduced risk of AKI and CNS dysfunction post op, although primary outcome of SIRS and organ dysfunction wasn’t different in these groups. In another study evaluating the effect of higher target BP in patients with prior hypertension, sublingual microcirculation (assessed by sidestream dark field imaging) significantly improved in patients with higher MAP. Given these observations, and the existing data from large RCTs, normalizing (rather than controlling) blood pressure in patients with chronic hypertension is not only unnecessary but can be harmful and the brunt of this harm is borne by the kidney.
Mean Perfusion Pressure (MPP) is given by the difference between Mean Arterial Pressure (MAP) and Central Venous Pressure (CVP) i.e. MPP=MAP-CVP. Another factor that can further compromise MPP in patients with CKD is increased CVP as a result of volume overload, diastolic dysfunction, and increased left and right ventricular filling pressures. This factor is likely to become more prominent with progressive GFR decline. Although KDIGO 2021 BP targets don’t apply to patients on dialysis, in this population the safe targets are likely to be further higher as highlighted by this pilot RCT.
Is the quality of evidence and strength of recommendation 2B or 2C?
KDIGO has graded the evidence supporting intensive BP lowering in CKD as 2B-a suggestion based on moderate quality evidence. We evaluated the evidence in the framework of GRADE, and reached a conclusion that evidence supporting this target is 2B at the best, a suggestion based upon poor quality evidence. Several features of the trials make the case for this:
1. Evidence supporting this is indirect (subgroup analysis and not an independent trial, now, someone may argue that it’s largest in terms of number, but it also is farthest from true CKD in terms of patient characteristics!)
2. There is risk of bias as trials considered are open label
3. Inconsistency of the observations -previous large trial, ACCORD BP, has refuted the hypothesis that intensive BP lowering helps
After having discussed potential risks of the intensive BP lowering, and lack of adequate evidence, and evidence of harm in patients with diabetes, strangely, guidelines have resorted to follow the intensive BP lowering. They applaud SPRINT’s plan of including CKD (GFR 20-59ML); however forget the fact that they ultimately ended up with a participant group with eGFR >70ml ( serum creatinine ~1 mg/dl). Unlike AASK and MDRD trials who also were set out to include patients with CKD and actually included them, SPRINT couldn’t enroll a real world CKD population. The reasons for selective inclusion of patients with higher GFR in SPRINT are unclear but one of them may be the perceived risk of intensive lowering in patients with lower GFR by the site physicians.
Summary
In the vast majority of the CKD patients in nephrology OPDs, evidence to lower BP target of <120 is nonexistent, and therefore guideline recommendation of <120 is not supported by the good evidence. With progressive decrease in kidney function, you get to the nephrology dark room where no evidence to guide BP management exists. Nephrologists, therefore shoulder the responsibility of treating one of the most difficult blood pressure challenges with no or little evidence to base their decision upon.
After careful evaluation of the available evidence, one would rather choose to maintain the equipoise about BP goal and individualize it for different situations after shared decision making with the patients.
Hydrochlorthiazide: the turtle of the race? “Adalphane Acedrex (a Novartis made combo of Reserpine+Dihydralazine+Hydrochlorothiazide)- was available in the hospital formulary and ‘uncontrolled hypertension’ was a rare condition”, Prof Hase would get nostalgic and remark on his grand rounds discussing evolution of pharmacotherapy for hypertension.
One of the earliest classes of antihypertensives, thiazide diuretics, are also one of the most effective drugs, with latest trial evaluating chlorthalidone showing a BP decline of almost 10mmHg. However, whether chlortalidone should altogether replace hydrochlorothiazide is still a matter of debate. This is an attractive proposition given the higher potency and some pleotropic benefits attributed to chlorthalidone (the term ‘pleotropic effect’ awakens sleeping skeptic in us, as this term is typically invoked to defend something that can’t stand scientific rigor alone). Large observational studies and meta-analyses have differing conclusions waiting for a randomized trial to settle the debate. (see here, here and here)
In a pragmatic randomized controlled trial involving 13,523 patients over 65 years of age, getting treated at Veterans Affairs health system, a switch to chlorthalidone (hydrochlorothiazide was the default thiazide at baseline), 12.5 or 25 mg did not improve the primary composite outcome of nonfatal myocardial infarction, stroke, heart failure resulting in hospitalization, urgent coronary revascularization for unstable angina, and non–cancer-related death. Primary outcome occurred in 702 patients [10.4%] in chlorthalidone and 675 patients [10.0%] in the hydrochlorothiazide group (hazard ratio, 1.04; 95% confidence interval, 0.94 to 1.16; P=0.45). The incidence of hypokalemia was higher in the chlorthalidone group than in the hydrochlorothiazide group (6.0% vs. 4.4%, P<0.001).
This trial is long-awaited evidence to understand the difference between two commonly used thiazide diuretics for the treatment of hypertension and reassures those physicians who haven’t yet switched to chlorthalidone. The superior efficacy of chlorthalidone to reduce blood pressure doesn’t translate into effectiveness. This trial is an example of low cost, operational research in the setting of structured heath care systems like VA. Such pragmatic trials are feasible, can be completed quickly (phenomenal recruitment rate of 100 patients per week!), and are possible at a substantially lesser cost.
Many hypertension clinics have already switched to chlorthalidone given the higher potency and 24-hour action of chlorthalidone. Both of these reasons are not good enough to inform practice. First, potency may not necessarily translate into efficacy (which current trial confirms). For example, immediate release nifedipine or hydralazine are potent antihypertensives but not necessarily effective at the ultimate goal of BP control-CV protection. Duration of action as well may not be valid argument as the mechanism of BP reduction with thiazides is unclear and both volume depletion and fall in systemic vascular resistance play a role. Modest vasodilatation observed with these drugs is more pronounced with chlorthalidone but contribution of this to the long-term BP reduction may not be substantial to change hard clinical endpoints.
Baxdrostat: new drug to treat hypertension
Hypertension is ‘the disease of kidney’, hypothesis that is supported by the fact that one of the most effective antihypertensives exert their effect via kidneys. Here is a welcome addition to the antihypertensive armamentarium —baxdrostat-a highly selective aldosterone synthase inhibitor. Prior efforts to inhibit this key enzyme in aldosterone synthesis were thwarted by concomitant and undesirable inhibition of cortisol synthesis catalyzed by 11 beta-hydroxylase (which share 93% sequence similarity with aldosterone synthase).
In this phase 2 trial-BrigHTN, 248 patients with treatment resistant hypertension were randomized to receive baxdrostat (0.5 mg, 1 mg, or 2 mg) once daily for 12 weeks or placebo.
Treatment resistant HTN was defined as: stable doses of at least three antihypertensive medications (one of which was a diuretic) and had a mean blood pressure of at least 130/80 mm Hg (the average of three measurements obtained with the use of an automated in-office blood-pressure monitor).
Trial was stopped early as criteria for overwhelming efficacy were met-a substantial decrease in blood pressure was noted with treatment: difference between the 1mg group and the placebo group, −8.1 mm Hg, and difference between the 2mg group and the placebo group, −11.0 mmHg, but the difference between the 0.5mg group and placebo was not significant.
Resistant hypertension is associated with high morbidity and mortality; baxdrostat is a welcome addition to our armamentarium to manage this condition. Some caution is needed before we consider it as a breakthrough. First, office BP measurements (primary endpoint) were used to assess the efficacy-why on the earth a Pharma who is able to pioneer a drug development can’t afford to use gold standard 24-hour ABPM to assess efficacy, when it is already used widely in practice? Second, there unexpectedly large placebo effect (9-10mmHg). The reasons for this may be multiple and given the office BP measurements used white coat effect is possible. For the same reason, patients with pseudo resistant HTN might have got enrolled. Factors like adherence to salt restriction, drug adherence, optimization of other antihypertensives might have decreased blood pressure in placebo arm as well as the drug (Hawthorne effect). More elderly patients got randomized to placebo; did it put control arm at disadvantage? This difference will be more relevant in long term, when CV outcomes of these patients will be compared. Phase 3 trials, involving larger sample size, longer follow up, and hard CV outcomes will clarify the pace of this agent in hypertension treatment.
Rise and fall of the sympathetic denervation in the treatment of hypertension
In patient on triple drug combination of CCB, ARB and thiazide, additional reduction in the BP after renal denervation was modest at 2 months. 136 patients with resistant HTN were randomized to ultrasound guided renal denervation-uRDN-(n=69) or a sham procedure (n=67). Primary outcome of reduction in daytime ambulatory systolic blood pressure was more with intervention than the sham procedure (-8·0 mm Hg [IQR -16·4 to 0·0]vs -3·0 mm Hg [-10·3 to 1·8]; median between-group difference -4·5 mm Hg [95% CI -8·5 to -0·3]; adjusted p=0·022). This difference persisted at six months as documented in this prespecified follow up analysis; however was diminished as compared to that noted at 2 months: mean daytime ambulatory BP at 6 months was 138.3 (15.1) mm Hg with uRDN vs 139.0 (14.3) mm Hg with sham (additional decreases of -2.4 [16.6]vs -7.0 [16.7]mm Hg from month 2, respectively).
Authors, nonetheless, are happy about fewer medication usages (although this difference wasn’t statistically significant at 6 months), and lesser need of aldosterone antagonists in intervention arm (hardly a reason to celebrate).
Renal denervation trials are classic example of the “big bang effect ” of scientific innovations. SIMPLICITY 1 and SIMPLICITY 2 reported a phenomenal reduction in BP over 30mmHg (for a moment elevating blood pressure of hypertension pharma). This was a massive overestimate, confirmed by SIMPLICITY 3 that addressed the key flaw of not having a sham control group in previous studies. We thought of waving a goodbye to renal denervation after these results.
But authors of the simplicity 3 want us to walk back in time and believe that the large reductions in BP reported by previous studies are supported by their 36 months follow up data of simplicity 3 trial published by lancet. The change in 24 h ambulatory systolic blood pressure at 36 months was -15·6 mm Hg (SD 20·8) in the renal artery denervation group and -0·3 mm Hg (15·1) in the sham control group (adjusted treatment difference -16·5 mm Hg [95% CI -20·5 to -12·5]; p≤0·0001).
There are more than one reasons not believe this tall claim: first, after unmasking at 6 months study didn’t remain a blinded trial and all the patient and physician related biases can cloud the conclusions. As highlighted by the editorial and a letter, Hawthorne effect- change in the behaviour of physicians (better monitoring, frequent reassessments) and patient (better compliance to dietary restrictions and medications) in the intervention arm can explain the apparent difference. Second, despite having uncontrolled hypertension, control arm didn’t receive additional medications to optimize control (did they punish participants refusing to cross over?). Several important questions are raised by this interesting letter as well.
Another confusing feature of this post trial follow up data was the choice of the comparator group, and the way BP measurements were done for this group. After 6 months, a large majority (101 of 171) of the patient crossed over to intervention, however as one might have expected, authors didn’t compare those who received denervation with those who didn’t. Instead, they considered cross over patients (along with those not crossed over) with their BP at 6month considered for final assessment (last observation carried forward). This further adds to difficulty in interpreting the effect of intervention versus placebo and makes assessment of true effect size difficult.
Lost and found theme has created a large number of Bollywood blockbusters, where lost brother or sister is brought back by the director after plot starts getting dull to add life to the story. Producer/director of SIMPLICITY 3 (Medtronic) tries this, but this is hardly enough to bring back this intervention in hypertension practice. There is no easy way to know the contribution of sympathetic over activity in an individual patient with hypertension and if such measures become available, we may be able to better define the role of this treatment. Until then, results of 36 months follow up can be taken with a pinch of NaCl.
Na restriction works to lower BP , may take potassium’s help
BP control doesn’t always need more drugs or interventions like denervation, sometimes smart and simple interventions can yield significant benefits. Two recent studies highlight this point clearly. Salt restriction can prevent age associated increase in blood pressure (age is no more a non-modifiable risk factor), controls BP in those who are already hypertensive and has huge potential to save lives. Salt restriction is the default advice that most hypertensive patients in our clinic receive but it easier said than done. With rapidly changing food environments, adhering to salt restriction is more and more challenging, controlling salt intake in clinical trial can be difficult. These group of investigators from China in their DECIDE-Salt trial played a smart trick.
48 residential elderly care facilities in China (1,612 participants including 1,230 men and 382 women, 55 years or older) were cluster-randomized using a 2 × 2 factorial design to provision of salt substitute (62.5% NaCl and 25% KCl) versus usual salt and to a progressively restricted salt intake (You can fool your taste buds and slow reduction in the salt intake can go unnoticed) versus usual supply of salt or salt substitute for 2 years. Salt substitute compared with usual salt lowered systolic blood pressure (–7.1 mmHg, 95% confidence interval (CI) –10.5 to –3.8), meeting the primary outcome of the trial, whereas restricted supply compared with usual supply of salt or salt substitute had no effect on systolic blood pressure.
This degree of reduction in BP is clinically relevant and is equivalent to adding one antihypertensive. Fewer cardiovascular events were noted in salt substitute group (hazard ratio (HR) 0.60, 95% CI 0.38–0.96), but this had no effect on mortality (HR 0.84, 95% CI 0.63–1.13). As expected, salt substitute increased biochemical hyperkalemia, but this was not associated with adverse clinical outcomes. Results confirm the findings of a previous large SSaSS trial which evaluated effect of this intervention in hypertensive rural Chinese population with past history of stroke. Greater reduction in BP (than SSaSS trial) is attributed to “better modulation” of diet in collective living setting where residents have limited control over the composition of the food they eat.
Important finding of the study was no effect of ‘progressively restricted salt intake’ strategy, which authors attribute to reliance on facility manager and cooks to deliver this (whom residents could influence), and the possibility that residents might have identified the food with restricted salt (buds used to a very high salt intake) and resorted to usual salt intake. Whatever may be the reason, this highlights the difficulty of implementing salt restriction at community level.
Predominantly men and Chinese population, lack of complete follow up data from one particular site, lack of 24-hour urine collection to ascertain the delivery of the intervention are the notable limitations. However, this study is a welcome and important addition to the efficacy and feasibility of sodium restriction as an intervention in hypertension.
STOPACE trial
Medical reversal -where in an established practice/treatment is proved either useless or, sometimes, harmful when subjected to rigorous testing by an RCT- is a regular occurrence in medicine. One classic example of this in nephrology was targeting higher hemoglobin in dialysis patients. This practice was proved harmful after many years when subjected to rigorous scrutiny by well designed RCTs. Stopping ACEi with advancing CKD may be another. This practice was based on hunch of the physicians and observational data . Even clinical practice guidelines are silent on what to do with RASi in advanced CKD. With no guidance and data, it was left to whims and fancies of treating physicians to decide regarding use of RASi in advanced CKD. We now have better evidence that stopping RASI may not be the right thing to do in advanced CKD.
STOP ACEi trial randomized 411 patients with advanced and progressive CKD (GFR<30ml/min) either to discontinue or to continue therapy with RAS inhibitors. The primary end point was the eGFR at 3 years. The difference in eGFR at 3 years was not different in the two groups (difference, −0.7ml/min; 95% CI, −2.5 to 1.0; P=0.42). Other important outcomes like ESKD, initiation of dialysis and CV events were no different in both groups.
The trial results are important in many aspects. It breaks the strongly held dogma that RASi must be withheld in advanced CKD. The trial enrolled real world advanced CKD: median age- 63 years, median serum creatinine-3.4mg/dl, median GFR-18ml/min, 29% patients had GFR<15ml/min, and 37% were diabetics.
The findings of the trial do not support the practice of STOPPING RASi in advanced CKD to improve kidney function. But what about effect of RASi on CV outcomes in advanced CKD? Well, there are no data in advanced CKD patients. Observational data suggests an association between increased CV events after discontinuing RASi.
With this study, it is prudent to continue RASi in advanced CKD and it’s time to move from “hunch” based medicine to evidence-based medicine!
EMPA-CKD trial
After iron and iodine, a day is not far when Flozins will be added to the list of food fortifications. That might be an exaggeration. But after securing a star status in management of DKD and heart failure, flozins are all set to stamp their authority in management of CKD patients.
EMPA CKD randomized 6609 CKD patients to empagliflozin or placebo. Enrolled patients had an eGFR 20 to 45 ml/min/ 1.73 m2, or who had an eGFR of 45 – 90 ml/min/ 1.73 m2 with a urinary ACR >200(mg/gm). After median 2 years of follow up, progression of kidney disease or death from cardiovascular causes occurred in 432 of 3304 patients (13.1%) in the empagliflozin group and in 558 of 3305 patients (16.9%) in the placebo group (hazard ratio, 0.72; 95% CI, 0.64 to 0.82; P<0.001).
Of the patients enrolled mean age was 63.8 years, non-diabetics were 54% and 35% had eGFR<3oml/min. Serious adverse events were not different in the groups. The patient population is more like what we see in CKD clinics. EMPA CKD trial in addition to DAPA CKD trial defines the role of flozins in CKD. Benefits were not significant in those without albuminuria (was it due to premature termination of the trial?) and in this patient subgroup further evaluation of these agents is needed.
Heterogeneity of response to treatment of hypertensive
One of my patients with CKD is a tailor and his chief complaint in the last clinic visit was his shrinking business in the era of ‘readymade’. Now a days, it is far more convenient to order online or buy readymade trousers from showrooms. I was wearing such a ‘readymade trouser’ in my cousin’s wedding, and everyone was staring at me instead of the newlyweds on the dais. I had just started feeling elated at my youthfulness, when my smarter half (wife) revealed to me that I was appearing a clown. ‘One size fits all’ approach is disastrous whether its clothing or medicine.
Everyone has experienced this phenomenon in our patients with hypertension; some people respond better to some medication than other. In this interesting and intelligently designed study, authors explored this question in a randomized double blind multiple cross over trial.
280 patients (median age 64 yrs, grade 1 hypertension) were randomized: Each participant was scheduled for treatment in random order with 4 different drugs (from 4 different classes): lisinopril, candesartan, hydrochlorothiazide, and amlodipine with repeated treatments for 2 classes. Each treatment period consisted of one week placebo washout, 2 weeks of dose escalation period, and at least 4 weeks of target dose period. 1468 completed treatment periods were evaluated and significant difference in BP responses were observed: Specifically for choices of lisinopril versus HCTZ, lisinopril versus amlodipine, candesartan versus HCTZ and candesartan versus amlodipine. Personalized approach can achieve BP reduction equivalent to half of that expected from single agent in monotherapy, and half of that expected after adding second agent. While some clinical characteristics are often used practically to decide which drug to start with, they are crude at the best. Laragh has proposed individualization based on plasma renin activity and classified drugs acting on renin axis – R drugs (RAS blockers, beta blockers, sympatholytics) or volume axis of hypertension V drugs (duiretics, CCBs, alfa blockers) and proposed to use drug from two difference classes in combination. This study shows that such approach is not only pathophysiologically appropriate but also produce clinically meaningful effect in BP management.
Since that embarrassing incident at my cousin’s marriage, I get all my trousers from my tailor friend, and he is just amazing. Hypertension, makes one of the good cases for personalized medicine-tailoring.
Precision medicine is the ‘talk of the town’ and our oncology colleagues, armed with an array of markers, genomics, proteomics, etc; often mock us for being ‘specialists’ farthest from ‘precision’. The eGFR-basic tool recommended for kidney function assessment epitomizes this imprecision. We have discussed eGFR and its limited utility in day-to-day practice in our previous post. As there is little doubt about its limited accuracy, the question is ‘how inaccurate is eGFR?’ In, what may be called one of the largest studies on mGFR-eGFR comparison, individual-level inaccuracy in eGFR was quantified in 3223 patients from 4 different patient cohorts. The results hopefully will make the nephrology community and guideline developers reexamine their overreliance on eGFR and CKD staging based on it. The following tables give a glimpse of this inaccuracy which is too large to continue relying on eGFR in practice.
eGFR
mGFR range
50%
80%
95%
60ml/min
52-67ml/min
45-76ml/min
36-87ml/mim
30ml/min
27-38ml/min
23-44ml/min
17-54ml/min
Possible mGFR ranges for eGFR 60 and 30 ml/min
mGFR>60
mGFR <45
eGFR 45-59ml/min
36%
20%
mGFR >30
mGFR <15
eGFR 15-29 ml/min
30%
5%
Chance of mGFR falling out of the eGFR range
The addition of cystatin C didn’t improve this inaccuracy substantially. Given these results, it wasn’t surprising that there was substantial disagreement in CKD staging by mGFR and eGFRcr. For example, you may consider referring somebody for AVF creation based on eGFR 20 ml/min, only to be embarrassed by the mGFR value of 39ml, which may be enough kidney function for patient’s lifetime.
For population-level interventions, eGFR may be an excellent metric. Population-level differences between mGFR and eGFRcr were small; the median difference (mGFR-eGFR) was 0.6 (95% CI, 1.2 to 0.2); however, for individual patient care, it is useless and may potentially be misleading. For the labs that automatically report eGFR alongside serum creatinine, now they should also incorporate the range of possible eGFR values, which will sound something like this: Mr Bean your serum creatinine is 1.3 mg, eGFR is 60ml, and this may correspond to the actual GFR anywhere between 36-87 ml. If labs start doing this (which is warranted by this study results) patients and clinicians will eventually stop paying any attention to this number. If you are reading this eGFR review, better to know beforehand that probably, it’s time to retire Mr eGFR.
2. Surgical treatment of asymptomatic kidney stones
Small (<6mm), asymptomatic kidney stones are typically treated conservatively. In this randomized controlled trial involving 73 patients who underwent surgery for a primary stone (one producing symptom /obstruction/considered high risk for an adverse clinical event) were randomized to receive clearance of secondary stones [defined as small (≤6 mm), asymptomatic renal stones that were located in the contralateral kidney (in the case of a primary renal stone) or either kidney (in the case of a primary ureteral stone, with the specific kidney identified before randomization]. At the end of 4.2 years of follow-up, the intervention arm had significantly lower relapse rates (hazard ratio, 0.18; 95% CI, 0.07 to 0.44), and a longer time to relapse(1631.6±72.8 days vs. 934.2±121.8 days). This exercise added only a little additional surgical time (25.6min) and was not associated with additional ED visits post-procedure.
The trial has limitations. It was open-label, small in size, had few non-white patients, and involved skilled endo-urologists, limiting the generalisability of these results in real life. Details of the medical evaluation and management to prevent recurrence aren’t available, leaving open the question if some of these recurrences were preventable. However, it’s not unusual to encounter a patient who has undergone half a dozen procedures for stones without even checking the serum calcium and phosphorus once – forget about the detailed evaluation (despite such harsh reminders). Most importantly, stone disease in our patients poses risk of life threatening sepsis, AKI and ESRD. This is unlike much of the developed world where it’s mainly the pain that bothers patients with nephrolithiasis.
Symptomatic primary stone disease in many patients is not addressed in time (cost and availability of expertise)and unfortunately remains one of the leading causes of ESRD and wider access to evaluation and intervention is urgently needed.
3. Role of steroids in Infection-related glomerulonephritis
The role of high-dose glucocorticoids in bacterial infection-related IRGN remains unproven. Bacterial IRGN can occur after a bacterial infection or in presence of an ongoing bacterial infection. Not only the utility of steroids is unproven, but their use also carries serious potential risks. This open-labelled study conducted at an academic center in India compared steroids added to supportive care versus supportive care alone.
Fifty-two patients with biopsy-proven infection-related glomerulonephritis and serum creatinine greater than 1.5 mg/dL were randomized to receive corticosteroids plus supportive care (intervention arm) or supportive care alone (control arm) and were followed for 6 months. Patients randomized to the intervention arm were given intravenous methylprednisolone, 1 g daily, for 3 consecutive days. This was followed by oral prednisolone 1 mg/kg/day for 1 month, followed by a slow taper at 5 mg/week. The primary outcome was complete renal recovery(eGFR>60ml/min) at 6 months.
At 6 months, there was no difference in the primary outcome in both arms.17 of 26 patients (65.4%) in the intervention arm and 14 of 26 patients (53.8%) in the control arm had complete renal recovery (odds ratio 1.6; 95% confidence interval [CI], 0.5 to 4.9; P = 0.397). However, there was a significant increase in adverse events in the steroid group. Adverse events occurred in 12 patients (46.2%) in the intervention arm and 2 patients (7.7%) in the control arm (P=0.002).
Authors should be commended for conducting such trial to fill an important knowledge gap. Apart from obvious design issues like open-label and single-center study, there were several other serious limitations of the trial. The trial was not prospectively registered and was underpowered as the sample size fell short of the intended 91 patients which were calculated to provide 80% power to detect a difference of 20% in primary outcome. Though this trial is a welcome addition to define the role of steroids in IRGN, the high risk of bias in the trial will not allow any definitive conclusions regarding the role of steroids in IRGN.
4. Diamox (acetazolamide) is back
Diamox (acetazolamide as a diuretic in the presence of metabolic alkalosis), Deviry (progesterone as a respiratory stimulant), and Deriphylline (oral bronchodilator) were three famous ‘Ds’ for managing hospitalised patients with ‘cor pulmonale’ when I was resident in internal medicine. Most of them are rarely used today, but acetazolamide is all set to make a big comeback with the publication of the ADVOR trial, which evaluated whether the addition of intravenous acetazolamide to standardized intravenous loop-diuretic therapy would improve the incidence of successful decongestion among patients with acute decompensated heart failure.
Of the 519 patients randomized, successful decongestion (primary outcome defined as the absence of signs of volume overload, within 3 days after randomization and without an indication for escalation of decongestive therapy) occurred in 108 of 256 patients (42.2%) in the acetazolamide group and 79 of 259 (30.5%) in the placebo group (RR, 1.46; 95% CI, 1.17 to 1.82; P<0.001). Other efficacy (death, readmission within 3 months) and safety outcomes (worsening kidney function, hypokalemia, hypotension, and adverse events) were not different in the two groups.
This study is a welcome addition (now the largest RCT of diuretics in HF)to the previously existing limited evidence to guide therapy in these settings. It brings back a forgotten diuretic that is economical and likely to be available widely. Although death rates reported are much lower than expected and were not different between the groups, decongestion is an important treatment goal in practice. Important limitations of the trial include the inclusion of only white patients, exclusion of newly diagnosed patients with HF, the control group receiving a fixed loop diuretic regimen (without scope to use infusion/higher dose/sequential blockade that is typically used in practice), and the lack of the current standard care with SGLT2 inhibition.
[P.S. curious thing about the protocol was the daily addition of half a liter of fluid -isotonic bicarbonate with magnesium supplementation- as maintenance fluid! Such maintenance fluid in patients with volume overload maintains only a congested state and patency of the IV line, and we are not sure about the latter.]
5. DIAMOND that didn’t shine as expected
The DIAMOND trial was planned to examine if the addition of potassium binder -patiromer will allow us to keep more patients on evidence-based therapy for heart failure -MRAs (mineralocorticoid receptor antagonists), ACE inhibitors, or ARBs-which is often limited by hyperkalemia. Less incidence of hyperkalemia—>more use of evidence-based therapy for HF—->improved survival/fewer hospitalizations with HF: this was a very attractive hypothesis of the DIAMOND trial, and the sponsors hailed the results as a breakthrough:
The efficacy of this drug to lower serum potassium was already documented in the OPAL-HK trial, and the goal of DIAMOND was to test the hypothesis of whether the addition of patiromer will permit wider use of evidence-based therapy of HF (ACE inhibitors, ARBs, MRAs) and thereby will bring about CV benefits. The original study end-point was robust: time to the first occurrence of cardiovascular death or cardiovascular hospitalization-which was modified due to the slow recruitment and pandemic situations to ‘mean change in serum potassium from the baseline’.
The pandemic was a hard time for running RCTs, and the authors should be congratulated for completing the trial, however, DIAMOND couldn’t demonstrate any of the hypothesized benefits of patiromer. At the median follow-up of 27 weeks involving 878 patients, the adjusted mean change in serum potassium was +0.03 mmol/l (95% CI–0.01, 0.07) in the patiromer group and +0.13 mmol/l (95% CI 0.09,0.16) in the placebo group, for a between-group difference of –0.10 mmol/l (95% CI –0.13, –0.07; P< 0.001). This hugely statistically significant difference in our opinion is clinically not meaningful. Authors made more than half a dozen comparisons for secondary and exploratory outcomes to make the same point of better control of hyperkalemia.
However, there are important lessons to be learnt from the results of this trial. Over 80% of the patients could continue the recommended doses of MRAs even in the placebo arm after having a history of hyperkalemia in the past, and this should caution against the practice of discontinuing the drug permanently after an episode of hyperkalemia (dose reduction or withdrawal followed by reinitiation is a better idea). Despite the clear benefit of the MRAs to reduce death and hospitalisations (RALES and EMPHASIS HF), only 15-30% of patients receive these drugs and one of the reasons may be knee-jerk reaction of stopping it permanently for hyperkalemia. As even the lower doses of these drugs are effective in reducing CV deaths and hospitalisations, DIAMOND trial showed that most patients can be maintained on MRAs even without patiromer.
More than 400 patients will need to be treated with patiromer for 3 years (which will cost about just 36000 USD) to prevent one MRA-preventable cardiovascular death or heart failure hospitalization, based on the results of the DIAMOND trial. One may wonder if wider use of other evidence-based agents like (Sacubutril/valsartan and SGLT2 inhibitors-both may attenuate the risk of hyperkalemia) may be more cost-effective than using patiromer indefinitely.
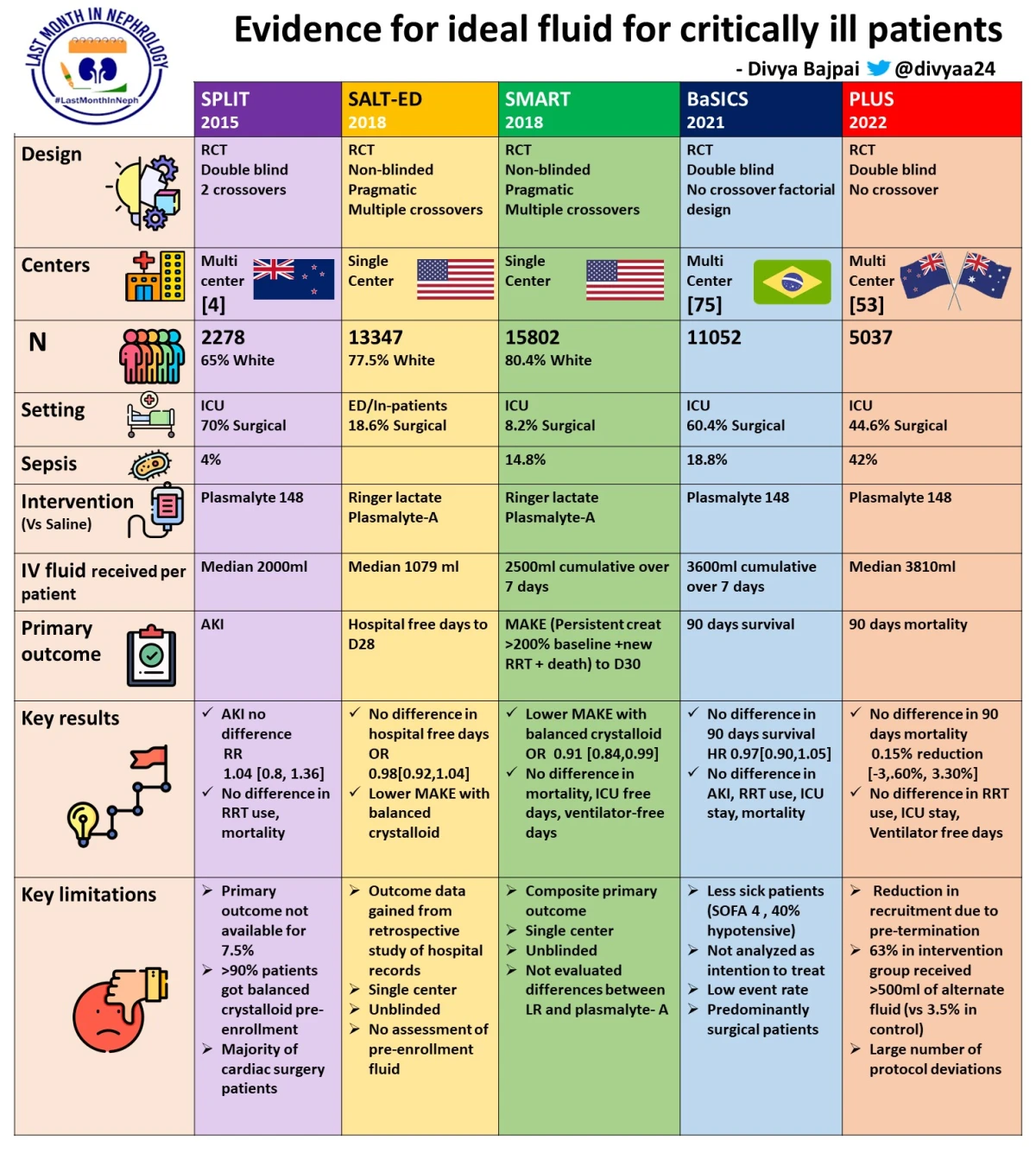
Indiscriminate intravenous fluid administration is extremely common, and nephrologists’ advice on fluid restriction often lands on deaf ears. Fluid management often becomes the battlefield involving intensivists, surgeons, and nephrologists. ‘Patient appears cool’ (when actually its the freezing air conditioner), ‘Skin turgor is poor’ (80-year-old lady, with dry and wrinkled skin for years, won’t glow up to pose for fairness cream ad), ‘BP isn’t picking up, give a bolus’ and so on! So many excuses! Most intriguing of all was this: I once asked a surgical fellow the reason for adding 1.5 liters overnight to the already massive positive fluid balance of a patient with pancreatitis, and he replied “my boss feels ‘cool’ about pushing in fluid”!
The harm of fluid overload has been clearly and consistently documented in children, post-operative surgical, and critically ill patients especially those on respiratory support for ARDS, leading to the default strategy of restricted fluid administration in many ICUs. While the beneficial effects of fluid restriction on lung function, and other surrogates like ICU stay were shown in previous studies, its effect on mortality is not clear.
The CLASSIC trial was set out to fill this evidence gap-1554 patients with septic shock (across 31 ICUs in 8 countries) were randomized; 770 were in the restrictive-fluid group and 784 in the standard-fluid group. 9.6 vs 11.1 L fluid was administered in the first week in restrictive and liberal arms respectively. At 90 days, death occurred in 323 of 764 patients (42.3%) in the restrictive-fluid group, as compared with 329 of 781 patients (42.1%) in the standard-fluid group (adjusted absolute difference, 0.1 percentage points; 95% CI −4.7 to 4.9; P=0.96). In the ICU, serious adverse events occurred at least once in 221 of 751 patients (29.4%) in the restrictive-fluid group and in 238 of 772 patients (30.8%) in the standard-fluid group (adjusted absolute difference, −1.7 percentage points; 99% CI, −7.7 to 4.3). At 90 days of follow-up, the numbers of days alive without life support and days alive and out of the hospital were similar in the two groups.
What do the results mean? Do they support liberal fluid administration? What do we take away to the bedside? Given the harm of volume overload and multiple trials showing no benefit of early aggressive fluid therapy (ARISE, ProMISe, ProCESS) restricted fluid administration is increasingly becoming a default strategy of fluid therapy. For instance, fluid administered in the first week following randomization has steadily declined over time: 17.6 vs 20.8 L in the 2006 FACTT trial, 12.4 L vs 13.6 L in the 2016 CLASSIC feasibility trial, and 9.6 vs 11.1 L in the 2022 CLASSIC final trial, in restrictive vs liberal arms, respectively. This ‘era effect’ is also evident from a study involving a national database of over 25000 patients with sepsis and septic shock, where fluid administered on day 1 was much lesser than that advocated by guidelines. Five-day cumulative positive fluid balance in the liberal fluid arm of THE 2006 FACTT trial (6.9L) is two times higher than in the 2022 CLASSIC trial!
Before you accept CLASSIC as the defeat of restrictive fluid strategy, wait. First, the results of the CLASSIC trial should be interpreted on this important background: change in the standard of care, which might have protected the control arm of the trial from the harm of fluid excess. Second, fluid administration is only one of the many interventions that can affect 90-day mortality in critically ill patients. The effect of these co-interventions is not clear from the published results. The CLASSIC trial thus no way refutes the harm of fluid excess (as claimed in the discussion section by authors) but rather reassures us that the restrictive fluid approach is feasible and safe. Another pitfall in most fluid trials is the assumption that all patients will be similarly affected (benefited or harmed) by a fluid administration strategy. “Fluid administration—->increased cardiac output—->increased O2 delivery——->increased O2 consumption” -this series of assumptions is the basis of fluid therapy. Many of these assumptions are not true in critically ill patients, for example, fluid bolus will increase cardiac output in only half of these patients. So this ‘one size fits all approach does not differentiate patients who are most likely to be fluid responsive from those who will be harmed by fluids. Therefore, future trials should assess the better metrics of fluid response (like increased cardiac output, or O2 delivery) to guide the fluid therapy. Let’s not forget that, in the setting of AKI, water is one of the most important uremic toxins, and restrictive fluid strategy becomes even more important.
2. Steroid treatment for IgA nephropathy
In many Asian countries, IgA nephropathy is the most common GN and an important cause of preventable ESRD burden and death. The need for prediction tools and appropriate therapies is more pressing here than anywhere else. The role of steroids in this condition is debated and their use is fraught with the risk of serious side effects as highlighted by the STOP IgA trial, and the initial report of the TESTING trial; immunosuppressed individuals with IgA nephropathy had an excess risk of infections, related hospitalizations, and death.
After getting halted by DSMB (due to the harm of immunosuppression), TESTING was resumed after 4 months, with modification of protocol: the dose of steroids was reduced to half the initial dose and TMP-SMX (cotrimoxazole) prophylaxis was added for infection prevention. 503 participants with proteinuria > 1 g/d, and eGFR of 20 to 120 mL/min/1.73 m2 were randomized (257 received methylprednisolone (MPS) and 246 received placebo, including 262 based on the original full-dose protocol and 241 based on the reduced-dose protocol). In combined results over a mean of 4.2 years of follow-up, the primary outcome-composite of 40% decline in eGFR, kidney failure (dialysis, transplant), or death due to kidney disease occurred in 74 (28.8%) vs 106 (43.1%) participants in the MPS vs Placebo (HR 0.53 [95% CI, 0.39-0.72]; P < .001).
TESTING is now the largest of the RCTs evaluating the role of the steroids in IgAN, and investigators should be applauded for pursuing the trial for over four years even after initial disappointing results. While TESTING takes steroids out of the ‘black box’, results pose several questions about the optimum utilization of steroids in this disease. Seemingly contrasting results of STOP IGA (showing little or no benefit of steroids and possible harm) may not be entirely explained by the racial/ethnic differences as proposed by the authors. A run-in phase, wherein non-immunosuppressive measures were intensified, was an important feature of the STOP IGA trial, and at the end of this phase, almost half of the participants which were initially thought to be candidates for immunosuppression (for proteinuria), achieved a significant decrease in proteinuria. The wider use of SGLT2 inhibitors may also further expand the scope of non-immunosuppressive treatment in this disease. Another puzzling characteristic of TESTING participants was a lower prevalence of hypertension (about 50%) as compared to the Indian GRACE IGANI (over 80%) cohort and STOP IGA participants (over 90% on RASi at enrollment and average requirement of 2-3 drugs for BP control). With relatively preserved renal function at enrollment, the TESTING control arm reported a higher rate of GFR decline (>5 ml per min/ year) than previously reported. TESTING participants were much younger than STOP IGA (~35yrs vs 43yrs), and excess risk of infections, hospitalizations, and death in these young patients is concerning when they may have excellent outcomes after dialysis/transplant. Unfortunately, many of these patients in developing countries still lack access to RRT and one of the reasons for starting immunosuppressives may be a desperate attempt to avoid dialysis at any cost, which can sometimes be a patient’s life.
TESTING has paved new hope for steroid use, however, it also leaves hard questions for future studies about the risk-benefit; hopefully, targeted-release form of the glucocorticoid-budesonide and other steroid-sparing strategies, histological predictors of response may help us better define the place of immunosuppression in IgA nephropathy.
3. The race for better eGFR equations continues If a poor common man tries telling you the truth, you silence him by telling him how ordinary and therefore unreliable he is. Then in search of the truth, we assemble a committee of multiple judges and assume their verdict as the best approximation of the truth. After having advocated, this ‘best substitute for truth’ for decades, we wake up on one fine morning, telling the world that we have been ‘not so correct’, and now the time has come to put another ‘good-looking guy’ in the assembly of judges to have a relook at the elusive truth.
Sounding like a Netflix courtroom drama, it’s the story of eGFR; where the director has decided to put another twist with the addition of smarter-looking guy ’Cystatin C’ to the existing CKD EPI equation. Retrospective individual patient data of 62 000 US adults ( 20 773 Black and 41 238 non- Black) enrolled in 8 well-characterized US cohort studies among the general population and among individuals with CKD were analyzed. Based on these data, the performance characteristics of 4 versions of the CKD-EPI equation were evaluated: (1) the original serum creatinine only– based CKD-EPI equation with the Black race coefficient intact (termed 2009 eGFRcr[ASR -Age,Sex, Race]); (2) a revised race-free serum creatinine only–based CKD-EPI equation (termed 2021 eGFRcr[AS]); (3) a previously developed race-free cystatin C only–based CKD-EPI equation (termed 2012 eGFRcys[AS]); and (4) the newly proposed race-free equation incorporating both serum creatinine and cystatin C (termed 2021 eGFRcr-cys[AS]). As expected, equation 4 showed a significantly higher prevalence of decreased kidney function in blacks at all levels of kidney function. So this equation allows one to eliminate race from the equation, a drive to eliminate racism from medical discourse.
IMHO, if you know serum creatinine well, with proteinuria and blood pressure it is enough for day-to-day clinical assessment of renal function, and apart from avoiding lawsuits (for example; you may be sued if gadolinium is given to a patient with eGFR 29ml/min and not if 31 ml/min), eGFR serves little purpose in routine clinical care. When checked yesterday, with twelve nephrology colleagues, none could recall using the eGFR calculator in the last week. Attempts to improve serum creatinine measurements are likely to impact the diagnosis and care of kidney disease much more than newer eGFR equations, more so in populations where none of the existing eGFR equations are formally validated.
After several decades of its use, efforts to improve the accuracy (decreasing analytic variations) of serum creatinine estimation are showing the desired results, with more and more labs reporting results traceable to IDMS international standards. Cystatin C will also need to be standardized before its widely used for eGFR equations and has its own limitations (check this Oct 2021 post for more on this). The new equation is likely to receive a grand welcome in KDIGO guidelines, which already have a 2C recommendation for cystatin c use.
Can experts now tell us “what was the contribution of the ’race factor’ in traditional eGFR equation to the late detection and overall poor CKD outcomes in blacks?”
4. Tebipenem of drug-resistant complicated urinary tract infection
The pace of developing antibiotic resistance far exceeds that of the discovery and clinical evaluations of the newer antibiotics. Global rise in MDR pathogens is a concern no lesser than melting glaciers and ecological collapse. It is commonplace to see a patient with pyelonephritis walking into the clinic (with little or no antibiotic exposure in past) with a scary antibiogram, showing none of the oral options valid, and not uncommonly ESBL producing gram-negative bug. Outpatient intravenous treatment has become a new norm now, which can be challenging due to the cost and resource constraints. This study is a much-needed addition to our antibiotic armamentarium, for the treatment of MDR uropathogens. In this phase 3, international, double-blind, non-inferiority, double-dummy trial, Tebipenem pivoxil hydrobromide (an orally bioavailable carbapenem with activity against uropathogenic Enterobacterales, including ESBL –producing and fluoroquinolone-resistant strains) was evaluated in 1372 hospitalized adult with complicated pyelonephritis. Overall response (58.8 vs 61.6%), clinical cure (93.1 vs 93.6%), and adverse events-most were mild- (25.7 vs 25.6%) were comparable between tebipenem and ertapenem. Welcome, Tebipenem.
Features common to ecologic collapse and antibiotic resistance are a lack of seriousness amongst clinicians, a lack of appropriate action (judicious and appropriate use), and a lot of plans at the bench with little action at the bedside. Nephrologists can play a definite role-pursuing surgery and physician colleagues to stop treating asymptomatic bacteriuria, avoiding treatment of CRBSI without cultures (this is an unfortunate culture in many dialysis units), and de-escalating to one (gram-positive or negative cover) as soon as possible while treating CRBSI or PD peritonitis.
5. Apixaban vs warfarin for treatment of VTE in patients on dialysis
It is challenging to use warfarin effectively in patients on dialysis. There are several challenges like drug interactions, time in therapeutic range, and inherent risk of bleeding in patients with CKD to name a few.
Direct oral anticoagulants (DOACs) are being increasingly used for thromboprophylaxis in patients with CKD. But there is no data about the safety and efficacy of NOACs/ DOACs in the treatment of VTE in patients on dialysis.
Wetmore et al conducted a retrospective cohort study using the United States Renal Data System data from 2013 to 2018. The study included dialysis patients who received a new prescription for apixaban or warfarin following a venous thromboembolism diagnosis. The outcomes were recurrent venous thromboembolism, major bleeding, and death. Of 12,206 individuals, 3130 were in the apixaban group. Apixaban, compared with warfarin, was associated with lower risks of both recurrent venous thromboembolism (hazard ratio [HR], 0.58; 95% CI, 0.43 to 0.77) and major bleeding (HR, 0.78; 95% CI, 0.62 to 0.98) in the intention-to-treat analysis over 6 months of follow-up. However, there was no difference between apixaban and warfarin in terms of risk of all-cause death (HR, 1.04; 95% CI, 0.94 to 1.16).
The majority of the cohort had DVT without pulmonary embolism.
There are several limitations. The article doesn’t mention the dose of apixaban used. While 2.5mg twice a day is approved in patients on dialysis, the RENAL AF trial, which is yet to be published, has used a dose of 5mg twice a day. It is unclear if the dose could affect the efficacy and/or safety outcomes. In the group that received warfarin, there is no information about INR or time in the therapeutic range. The study may have missed bleeding episodes managed in the emergency department.
Conducting an RCT comparing warfarin to DOACs will be a Herculean task. Till then we will have to make use of these data in shared decision-making.
1,3, 4 written by Tukaram Jamale and peer reviewed by Vaibhav Keskar, Manjunath Kulkarni and Divya Bajpai
2 written by Manjunath Kulkarni and peer reviewed by Tukaram Jamale, Vaibhav Keskar and Divya Bajpai
5 written by Vaibhav Keskar and Peer reviewed by Tukaram Jamale, Manjunath Kulkarni and Divya Bajpai
a) PLEX has no important effects on all-cause mortality, b) PLEX reduced the risk of ESKD at 12 months, and c) PLEX increased the risk of serious infections at 12 months.
These conclusions are just as definitive and helpful for clinicians as the monsoon predictions of our meteorologic department to farmers, and wise farmers take them just as seriously as the monsoon predictions based on the height of the crow’s nest on the tree.
This paper demands a major correction in the ’ what you already know on this topic’ section which reads: “clinicians use PLEX as a treatment in vasculitis based on the ’biological rationale’ and ’small clinical trials’-completely ignoring the significant practice change (of restricted PLEX USE) that followed PEXIVAS trial; the largest of the trials addressing this question.
The results of this review are largely driven by MEPEX and PEXIVAS trials. Although both were addressing the similar question, for many reasons, they aren’t comparable. Change in the standard of care over the long period of 13 years after the publication of MEPEX is likely an important issue underlying the differing conclusions of these trials: more use of IV CYP (giving the lower cumulative dose), use of lower dose steroids, and overall improvement in the care of patients with renal failure, might have left little room for PLEX in management in PEXIVAS trial.
The ancient question of ’ well-done RCT vs meta analysis’ has once again surfaced here and we prefer to side with the well-conducted large RCT instead of the meta-analysis combining studies of various sizes, designs, and strengths. PEXIVAS was a large and rigorously done RCT (reviewed by us in March 2020 post) after which it’s difficult to justify the routine use of PLEX in this disease. A recent large retrospective study also demonstrated the futility of PLEX in the contemporary population with ANCA vasculitis. Believers of PLEX point to limitations of the PEXIVAS trial: lesser severity of azotemia in its participants, the lack of data on histological severity, and possible benefit in patients with alveolar hemorrhage. Most of these arguments are held by dogmatic belief in the PLEX rather than the available evidence.
MEPEX
PEXIVAS
Total number of participants
137
704
Number on dialysis
137
140
Number with alveolar hemorrhage
31
191 (severe in 61)
The only major limitation of PEXIVAS may be the lack of histological data, which could have guided us about the histological correlates of response to PLEX, and the possibility of the benefit of the PLEX in the subgroup of patients with severe histological features remains unanswered.
What do we take away? A definite new message from this meta-analysis is that PLEX is an immunosuppressive strategy that can increase the risk of infections. How to trade off short-term benefits on kidney function with an increased risk of infections? This is a dilemma that clinicians are likely to face now. Bottom line: In a patient with biopsy suggestive of severe disease and poor response to the standard immunosuppression, one can engage in a discussion about the risks and benefits of the PLEX.
Hypertension and nephrologists
‘Hypertension is a disease of kidney’ Professor Hase would start his lecture on hypertension. Given the central role of the kidney in sodium and volume regulation, there is no exaggeration in saying that essential hypertension is ‘kidney failure without azotemia’. As summarised in this latest review in NEJM, seminal integrated physiology work by Guyton and colleagues, demonstrating the close relationship between sodium, volume, blood pressure and their regulation by the kidney remains valid after 50 years of its initial description and in spite of the challenges by alternative hypotheses of vascular dysfunction and immune system activation in the genesis of hypertension.
Over 80% of the patient with kidney disease have HTN, which reflects the close and bidirectional relationship of kidney function with blood pressure: with increasing severity of kidney disease, HTN gets more severe, and uncontrolled severe HTN drives the progression of kidney disease. Not surprisingly, very few specialists are confronted with ‘difficult hypertension’ like nephrologists, which makes them one of the best HTN specialists (not graded, huge personal COI).
Thanks to renalism, with the increasing severity of CKD, more and more renalism comes in and evidence guiding the hypertension treatment becomes weaker and weaker.
Agarwal et al are all set out to clear the clouds here, and after resurrection of atenolol for HTN in patients on dialysis their CLICK trial has now reported a remarkable reduction in blood pressure in a population which otherwise qualifies for exclusion in HTN trials.
160 patients with stage 4 CKD and uncontrolled HTN (most receiving 3-4 drugs at baseline to control BP, now that’s nephrologist’s HTN!), were randomized to receive chlorthalidone at an initial dose of 12.5 mg per day, with increases every 4 weeks if needed to a maximum dose of 50 mg per day, or placebo; randomization was stratified according to previous use of loop diuretics. The adjusted change in 24-hour systolic blood pressure from baseline to 12 weeks was −11.0 mm Hg (95% confidence interval [CI], −13.9 to −8.1) in the chlorthalidone group and −0.5 mm Hg (95% CI, −3.5 to 2.5) in the placebo group. The between-group difference was −10.5 mm Hg (95% CI, −14.6 to −6.4) (P<0.001). While the degree decrease in the blood pressure isn’t very different than that reported with major first line agents, its noteworthy that this was a population already on more than 3 drugs, and this effect is therefore remarkable. Significant reduction in albuminuria was also observed in patients treated with chlorthalidone group possibly due to diuretic-induced potentiation of antialbuminuric effects of renin–angiotensin system inhibitors.
Limited duration of follow up, small sample size, no inclusion of Asians, and lesser representation of women are notable limitations of the study which demands further large scale evaluation of this class of drugs in CKD HTN focusing on hard CV and renal endpoints. Nonetheless, long held dogma (based on an experimental study done in 1960s ), that thiazides are largely ineffective in treatment of HTN in advanced CKD is challenged by this study. CLICK trial is a welcome and long due addition to the limited evidence base to guide antihypertensive therapy in this population.
Sodium intake in heart failure(HF)
Like cirrhosis and nephrosis, HF is a state of poverty (reduced EABV)amidst prosperity (net salt and water excess) and one usually recommend sodium restriction of less than 3 gram per day to patients with heart failure. This recommendation is based on expert opinion and low-quality evidence. This leads ACC/AHA to recommend this:
Guideline in fact doesn’t use the word restriction and rather limits itself to ‘avoiding excess’ in the absence of any credible evidence on the benefit of sodium restriction. It is disheartening to note that one of the “cornerstone recommendations” for heart failure is based on flimsy evidence. Understandably there was a lot of excitement about the SODIUM-HF trial which attempts to answer this important question.
SODIUM-HF is an international, multicentre, open-label, RCT that enrolled 806 adult chronic heart failure who were randomly assigned (1:1) to either usual care or a low sodium diet of less than 1500 mg/day. The primary outcome was the composite of cardiovascular-related admission to hospital, cardiovascular-related emergency department visit, or all-cause death within 12 months. The investigators found the primary outcome had occurred in 60 (15%) of 397 patients in the low sodium diet group and 70 (17%) of 409 in the usual care group (hazard ratio [HR] 0·89 [95% CI 0·63–1·26]; p=0·53). They concluded that a dietary intervention to reduce sodium intake did not reduce clinical events.
SODIUM-HF set out to answer a vital question and based on the results, the authors emphatically claim: “study is the largest randomised clinical trial to test a strategy of dietary sodium reduction for patients with heart failure to date” and “study provides high-quality evidence to guide clinical decision making”. While the first half of the claim is true (trial is indeed the largest one on this topic), the second is far from the truth. Before getting carried away by the lofty claims of the authors, let’s examine the study in some more detail.
First, the study isn’t sufficiently powered to address the question. The authors assumed the event rate of 25% in the control arm and a relative risk reduction of 30%. The actual event rate in the trial was 15% and with this event rate, to detect a 30% reduction, we need 1722 patients. Also, over 50 patients discontinued study treatment for various reasons further compromising power. Second, the dietary recall method to check that intervention is adhered to is unreliable. In a single-blind(assessors were blinded) study, where patients were aware of the intervention, it’s likely to introduce ‘co-intervention’ where patients in the control arm can restrict the sodium intake blurring the separation in the groups. This can be inferred from the post-intervention median sodium intake in the two groups: 1658 mg/day (1301–2189) vs 2073 mg/day (1541–2900) in the intervention and control arms respectively. This wide variation in the intake of sodium in the control arm is suggestive of ‘contamination bias’. Moreover, the intervention arm was telephonically contacted more often (almost monthly), raising suspicion of the performance bias. Third, there seems to be major confusion about the amount of sodium prescribed to the participants, which differs in the protocol registered and the published paper-which everywhere wrongly equates less than 1500mg to less than 100mEq (when actually 1500mg equals 65mmol). Kudos to the reviewers of Lancet! Fourth, study protocol (supplementary appendix) talks of the primary endpoint assessment at 24 months, while paper reports it at 12 month, leaving us clueless as to the reasons of this change in the goalpost. Finally, not only the authors claim exact sodium intake based on recall, they also report the exact fluid intake (e.g.median intake 1782 ml). Ordinarily, thirst (and water intake) is inversely related to salt intake which was not observed in this study. We are also curious to learn their technique of quantifying fluid intake so accurately!
Given these issues, study only adds to the poor quality of the evidence on the salt restriction in heart failure.
We really enjoyed interpreting the published articles with the help of expert national and international faculty in this workshop. We had an overwhelming response from the delegates (370 + registrations) with interactive ‘Q and A’ sessions.
Did u miss the live workshop? Don’t worry we got you covered. Here is the recording of the program –
“Hyperchloremia produces progressive renal vasoconstriction and fall in GFR that is independent of the renal nerves, is potentiated by prior salt depletion, and is related to tubular Cl- reabsorption. Chloride-induced vasoconstriction appears specific for the renal vessels” reads the conclusion of the seminal paper by Christopher Cox published in JCI 1983. After a prolonged quiescence of almost three decades, the harm of saline became the topic of debate and discussion following the publication of this sequential period pilot study in JAMA 2012, which reported a dramatic reduction in the risk of AKI after switching to the strategy of chloride restrictive fluid administration. Although, we often consider this study as the starting point of this ‘fluid debate’, the guys who performed a small but elegantly done 2012 pilot RCT addressing this question were a group of surgeons, with rather aberrant research interest in fluid therapy (we often joke about their knowledge of renal physiology, especially fluids, but some of them can be really cool!).
A sequential period pilot study wasn’t considered definitive enough to change the practice, for several reasons like ‘before-after design’, the possibility of Hawthorne effect, and doubtful plausibility of its rather massive effect size (40% decrease in the risk of AKI). Several large trials were subsequently published examining the harm of (ab)normal saline (if you are a tonicity freak, who like to call saline abnormal): SPLIT (2015), SALT-ED & SMART (2018), BaSICS (2021), with the latest addition of PLUS trial (2022) which will be discussed here.
In this double-blind RCT, conducted across 53 ICUs in Australia and New Zealand, involving 5037 critically ill patients, 2515 patients were assigned to the BMES (Balanced Multi Electrolyte Solution) and 2522 to the saline. The primary outcome of death from any cause within 90 days was no different in BMES vs saline [21.8 (530 of 2433 patients) vs 22% (530 of 2413 patients), 95% CI −3.60 to 3.30; P=0.90]. Similarly, secondary endpoints-mainly renal-receipt of new RRT [12.9% (310 of 2394 patients) vs 12.7% (306 of 2403 patients) 95% CI, −2.96 to 2.56] and the maximum increase in the creatinine level during ICU stay (0.41±1.06 mg/dl vs 0.41±1.02 mg/dl) showed no difference.
How do we reconcile seemingly contradictory results of SALT ED, SMART vs SPLIT, BaSIC and PLUS?
Pragmatic trials are relatively simple and easy to conduct, more aligned with the standard clinical practice, can recruit a large number of patients over a shorter time span, and are considered to have higher external validity. However, they are best suited to examine ‘whether an intervention actually works in real life’ after an explanatory trial has shown ‘if and how an intervention works (BaSIC and PLUS were needed before SALT ED and SMART). One of the 9 essential PRESIC 2 characteristics of pragmatic studies is the choice of the primary outcome which preferably should be a patient-centered hard outcome. This is especially important when trials have a very large sample size and can detect the small difference in the outcome which may be statistically significant but clinically irrelevant. In the SALT ED trial, the primary outcome of hospital-free days didn’t differ between the groups, and renal benefits (MAKE) were assessed as the secondary outcome. While SMART assessed MAKE as the primary outcome, the difference observed was small and none of the individual components of MAKE was significantly different between the groups. More flexible conduct of the trial is also reflected by the smaller difference in the chloride concentrations (which is thought to medicate the harm of saline) between the groups in these trials when compared to BaSICS and PLUS trials where a better separation of serum chloride concentration was observed. Also, possibilities of Hawthorne effect and ascertainment bias are limitations of the open-label, pragmatic trials.
Summary of evidence on fluid of choice for critically ill patients.
BaSICS trial involving over 11000 patients (largest double-blind trial on the topic so far ) across 74 ICUs, failed to show any benefit of fluid type on survival and suggested the harm of balanced fluid in patients with head trauma. BaSICS was criticized for a relatively low event rate (decreased power) and predominantly surgical patients (limiting generalizability to other critically ill). Most of these concerns were addressed in the PLUS trial, which we believe may be the best available trial on this topic. It involved critically ill medical patients, achieved better separation of chloride levels (indicating stricter adherence to the study fluids), selected hard patient-centered outcomes, and remained adequately powered even when the trial was truncated due to the COVID19 pandemic.
A 2020 meta-analysis on this topic (which was largely driven by SMART trial), concluded: “resuscitation with balanced crystalloids demonstrated lower hospital or 28-/30-day mortality compared with saline in critically ill adults but not specifically those with sepsis. Balanced crystalloids should be provided preferentially to saline in most critically ill adult patients”. Although authors of the latest 2022 meta-analysis (including BASICS and PLUS trials) aren’t willing to accept the clinical equipoise, they are less definitive in their conclusion which goes like this: “The estimated effect of using balanced crystalloids versus saline in critically ill adults ranges from a 9% relative reduction to a 1% relative increase in the risk of death, with a high probability that the average effect of using balanced crystalloids is to reduce mortality“. Authors suggest not to take the frequentist’s stand and urge us to follow the Bayesian interpretation of the direction of the effect size, ignoring the confidence intervals that cross unity. In the perennial debate of ‘well-done RCTs versus meta-analysis putting together several studies of varied design, power, endpoints’, we place far greater weight on BaSICS and PLUS here.
What do we take to the bedside? There is no ideal ‘solution’ that will suit all the problems. The balance of this fluid debate stays neutral. Saline remains a valid first-line option for fluid therapy, in most critically ill patients. Patients with worsening hyperchloremia and acidosis after initial resuscitation may be offered balanced fluids. Balanced fluids should be specifically avoided in those with cerebral edema and can be preferentially used in patients with metabolic acidosis.
Mycophenolate after rituximab in complicated childhood nephrotic syndrome
Rituximab may be effective in prolonging remission in steroid-dependent or CNI-dependent patients. Its use is recommended in patients who have either failed CNI or have received these agents for a prolonged duration. Patients with complicated FRNS/ SDNS treated with rituximab experience relapses after recovery from rituximab-induced peripheral B cell depletion. Repeated rituximab infusions may work, but are fraught with serious adverse effects.
Japanese Study Group of Kidney Disease in Children conducted a multicenter, randomized, double-blind, placebo-controlled trial to examine whether mycophenolate mofetil (MMF) administration after rituximab can prevent treatment failure (FRNS, SDNS, steroid resistance, or use of immunosuppressive agents or rituximab)
Thirty-nine patients in each group were treated with rituximab, followed by either MMF or placebo until day 505 (treatment period). The primary outcome was time to treatment failure (TTF) throughout the treatment and follow-up periods (until day 505 for the last enrolled patient).
Time to treatment failure was clinically but not statistically significantly longer among patients given MMF after rituximab than among patients receiving rituximab monotherapy (median, 784.0 versus 472.5 days, hazard ratio[HR], 0.59; 95% confidence interval [95% CI], 0.34 to 1.05, log-rank test: P=0.07).
Secondary endpoint analyses revealed that MMF after rituximab decreased the relapse rate and daily steroid dose during MMF administration by 74% (HR, 0.26; 95% CI, 0.08 to 0.48) and 57% (mean ±SD: 4.45 ±3.52 versus 10.45 ±12.49 mg/m2 per day, P=0.0004), respectively.
However, after MMF discontinuation, the relapse-preventing effect disappeared, and most patients in the MMF group presented with treatment failure. To sum up, it is unclear if any maintenance strategy after initial rituximab therapy would result in any meaningful clinical benefit.
HIF-PHI drugs are effective, are they safe?
Daprodustat is an oral hypoxia-inducible factor prolyl hydroxylase inhibitor(HIF-PHI), which stimulates erythropoiesis and improves iron homeostasis. HIF-PHI drugs have the distinct advantage of being orally active. We reviewed PROTECT and INNOVATE trials last year.
Summary of recent trials about IHF-PHI safety
ASCEND-D and ASCEND-ND trials randomized dialysis (DD-CKD) and non-dialysis (ND-CKD) patients respectively to receive Daprodustat or an ESA. Both trials demonstrated non-inferiority of daprodustat with respect to change in hemoglobin level.
In DD-CKD, mean change in the hemoglobin from baseline to week 28 through 52 was 0.28 g/dl in the daprodustat group and 0.10 g/dl in the ESA group (difference, 0.18 g per deciliter; 95%CI, 0.12 to 0.24), which met the prespecified non-inferiority margin of −0.75 g per deciliter. Similarly, in ND-CKD the difference was 0.08g/dl, which met the non-inferiority margin.
Anemia trials have taught us to critically assess the safety of ESAs before approval. In DD-CKD, during a median follow-up of 2.5 years, MACE occurred in 374 of 1487 patients (25.2%) in the daprodustat group and in 394 of 1477 (26.7%) in the ESA group (hazard ratio, 0.93; 95% CI, 0.81 to 1.07), which also met the prespecified non-inferiority margin for daprodustat. The percentages of patients with other adverse events were similar in the two groups.
In ND-CKD, daprodustat was noninferior to darbepoetin alpha, both in efficacy and CV safety. With respect to MACE events, HR was 1.03(95% CI, 0.89-1.19). An important point to note here is: on-treatment analysis of CV safety favored ESA over daprodustat. The trial also raised other major safety concerns with daprodustat in the non-dialysis population. Cancer-related deaths, tumor progression, tumor recurrence, esophageal and gastric erosions were significantly more in Daprodustat group.
The question of the efficacy of the drug in treating anemia of chronic kidney disease is answered. However, the question of safety is not clear. In the ND-CKD population, this result of CV safety of ASCEND-ND is in sharp contrast to PROTECT trial. In PROTECT trial, vadadustat did not meet the non-inferiority criterion for CV safety. The reason for contrasting findings of PROTECT and ASCEND-ND is not clear. Results of CV safety in the non-dialysis population are less than convincing. Also, FDA analysis of roxadustat pooled data has raised safety concerns about CV safety in the non-dialysis population. There was a strong thrombosis signal in roxadustat arm. Also, significantly more cancer-related deaths in daprodustat arm of the ASCEND-ND trial are cause for concern.
‘Trial designs’ are important when analyzing safety data. Placebo-controlled trials offer a better opportunity to assess the safety of drugs. FDA analyzed safety in ND-CKD of roxadustat versus placebo and highlighted some safety issues. Moreover, the choice of safety margins in non-inferiority trials is arbitrary. There is no reasonable data to determine and justify the margin for safety. We also do not know if non-inferiority trial designs are appropriate to answer questions of drug safety. Given all these concerns, the safety of HIF-PHI in ND-CKD will still be a question.

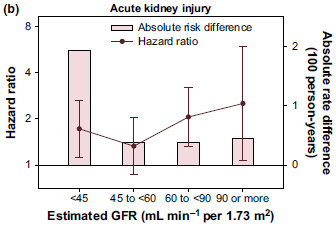







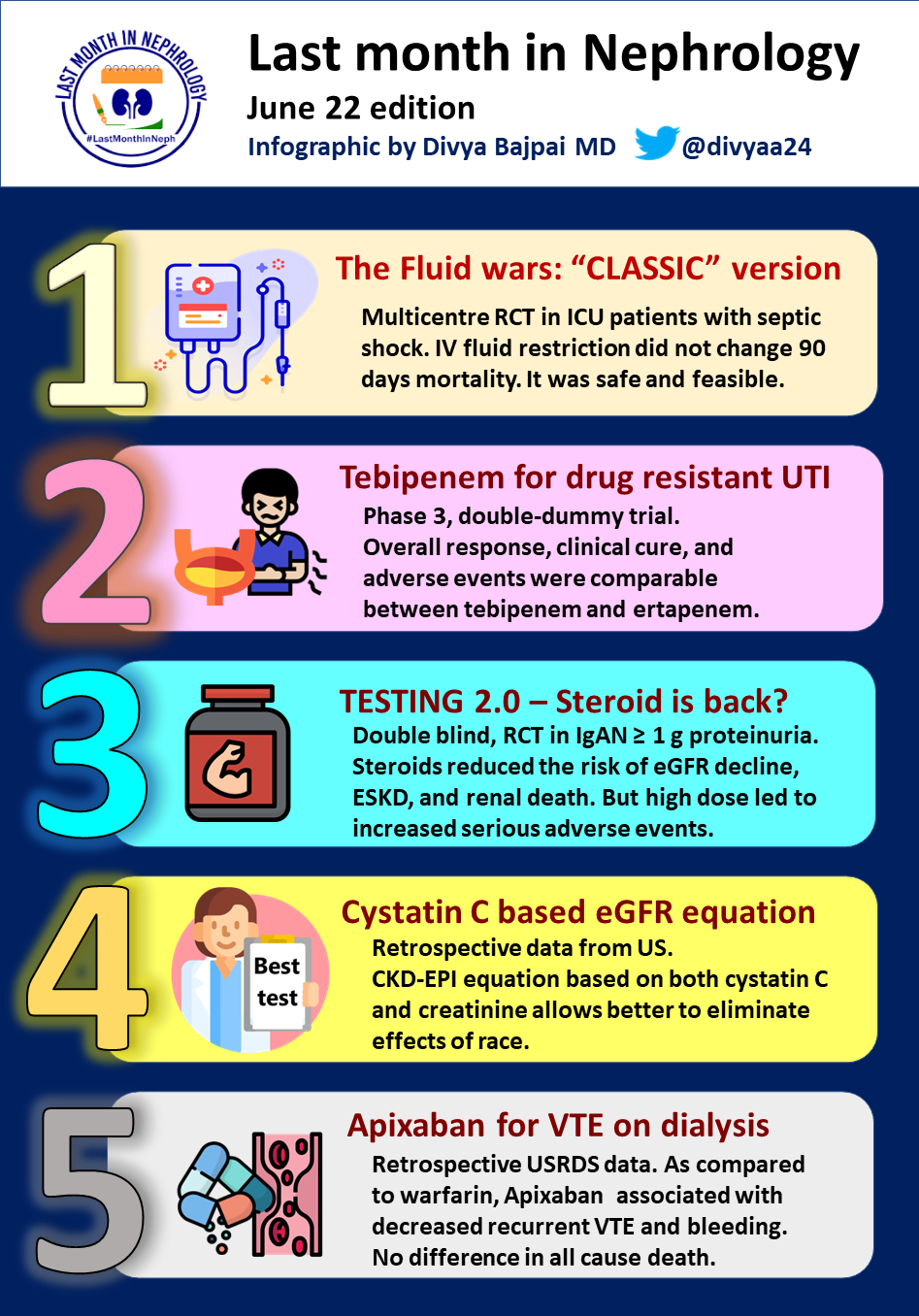



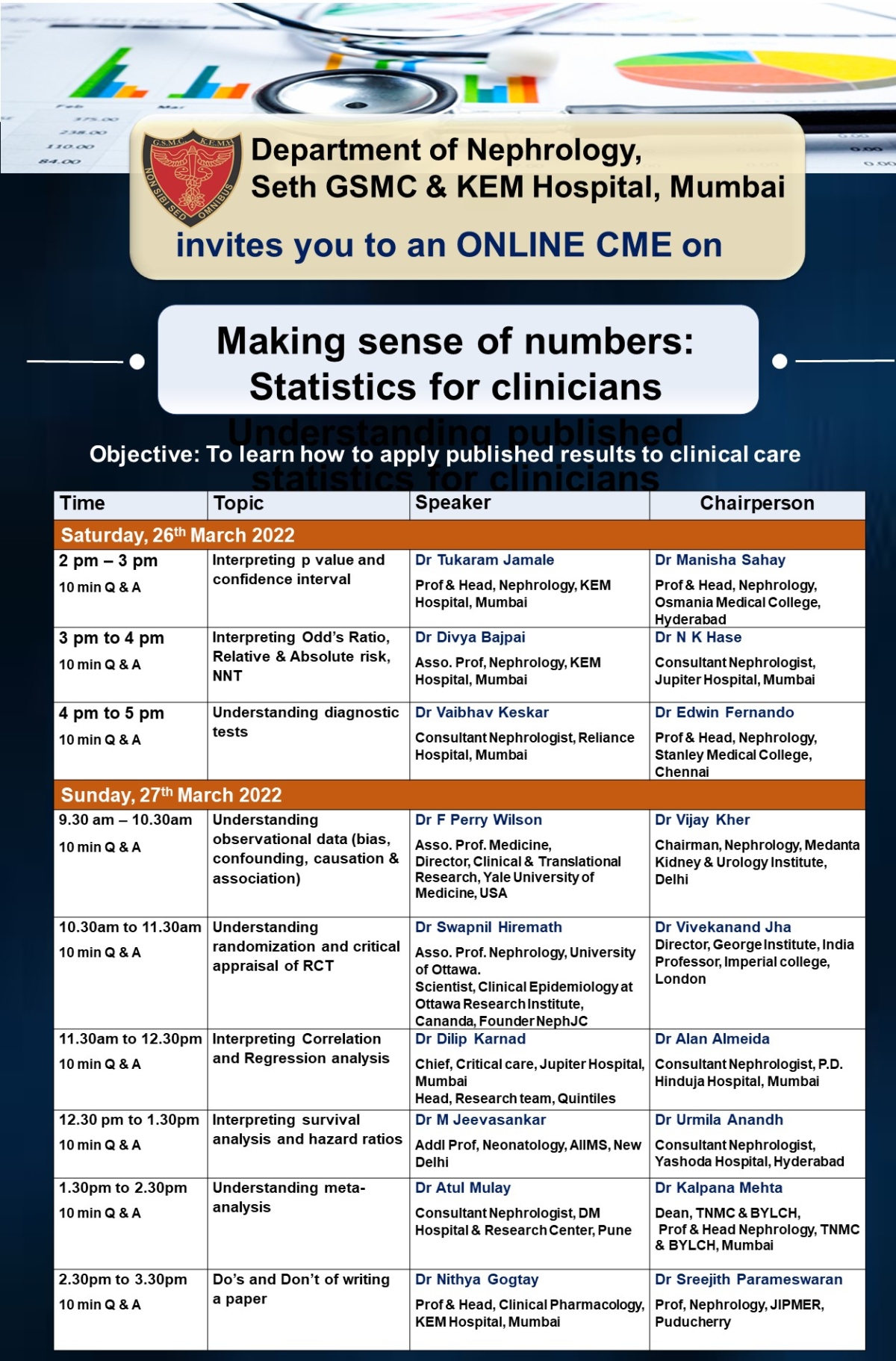
 ️Interpreting published Statistics for Clinicians
️Interpreting published Statistics for Clinicians